By Guest Author Lisa U. Kleinz, MA, SLP-L, CLC, CNT Director of Education, Dr. Brown’s Medical
What does the research tell us?
There has been much discussion recently on the flow rates of the artificial bottle nipples, due to varying reports in some of the most recent articles published on flow rates. In fact, there is a newly released article from the United Kingdom. (Abstract link: https://doi.org/10.1080/2050571X.2019.1646463)
Below is verifiable information to better interpret the research behind “nipple flow rates.”
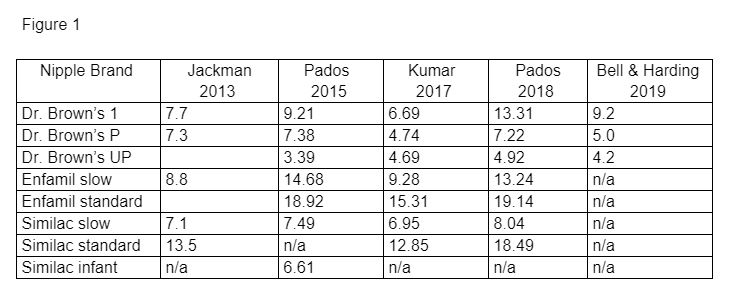
The most recent studies present different flow rates for all brands of nipples. (Refer to Figure 1 below.). In fact, all the most widely referenced published flow rate studies have varying levels of flow rates for the same nipples. Why? If the authors are testing the same nipples, why not the same results?
Reason #1 – Each study employs a different methodology to conclude their data. For instance, in the most commonly reported nipple flow rate studies, the suction pressure applied with a breast pump for liquid extraction varies with each.
Changes in the pressure applied to extract the liquid can influence the flow rate of all nipples used. This is especially true in a faster flow nipple, such as a level 1 nipple since the hole is larger than the slower flow nipples.
Reason #2 – The angle of the bottle is held at varying degrees.
Reason #3 – Each study tests a different number of nipples for each brand to determine the average flow rate and coefficient of variation.
Reason #4 – Some studies are testing the nipple flow rates with formula and some with water. The viscosity of the liquid being tested will alter flow rates.
Reason #5 – Collar “tightening” or “torqueing” will vary the pressure within the bottle system and can increase or decrease the amount of air allowed in the bottle system. If all bottles are not provided the same amount of torque when testing each nipple, the results will vary.
Reason #6 – If nipples that are intended to be used with a vented or vacuum-free system are tested in a bottle without the internal vent system, the true flow rates will not be established.
For ALL of the above reasons, it is recommended clinicians do not compare reported flow rates among different research studies. Clinicians may want to use an article as a general guide to determine how different nipples appear in relation to each other. It is difficult to determine exactly what the baby will receive when sucking on a bottle nipple because a breast pump is NOT similar in relation to an infant’s suck. Each infant applies different suction pressure when feeding. In the Pados 2018 article, the author states, ”the flow rates achieved using this standardized approach may or may not reflect the flow rate an infant would be exposed to when feeding with the nipple but can be used to evaluate the relative flow rate across nipple types.”
In addition to investigating flow rates of nipples, the coefficient of variation which reports on the consistency of nipples is important to consider when choosing a nipple for an infant. The clinician should look for nipples that have nipple flow rates that are consistent and reliable, with low coefficient of variables.
It is important to consider that all flow rate studies should NOT be used as a ‘be all/end all’ approach to finding the right nipple for a baby. These studies should be used as a guide to view the relative relationship of different nipples among each other, as well as to determine how reliable specific brands are. Remember – Flow rate matters. It is important for safety and for creating positive neuronal pathways. A culture that allows an infant to have a different experience with each new caregiver is no longer acceptable.
Feedings should be infant-driven, with careful attention to what the infant is telling us about a flow rate. By allowing the baby to communicate with feeding cues it allows us as clinicians to better interpret their cues and adapt a presentation of proper feeding tools.
To receive more information specifically about Dr. Brown’s™ Medical products, please go to www.drbrownsmedical.com
References
Bell N & Harding C. An investigation of the flow rates of disposable bottle teats used to feed preterm and medically fragile infants in neonatal units across the UK in comparison with flow rates of commercially available bottle tests. Speech, Language, and Hearing. 2019. DOI: 10.1080/2050571X.2019.1646463
Jackman K. Go with the flow: Choosing a feeding system for infants in the neonatal intensive care unit and beyond based on flow performance. Newborn & Infant Nursing Reviews. 2013;13:31-34.
Kumar R, Madden M. Lost and overwhelmed in the nipple aisle? A comparison of bottle nipple flow rates and viscosities for clinicians. Poster presented at Feeding Matters Conference, January 2017.
Pados B, Park J, Thoyre S, Estrem H, Nix WB. Milk flow rates from bottle nipples used for feeding infants who are hospitalized. American Journal of Speech-Language Pathology. 2015;24:671-679.
Pados B, Park J, Dodrill P. Know the flow: Milk flow rates from bottle nipples used in the hospital and after discharge. Advances in Neonatal Care. 2019;19(1):32-41.

 There has been much discussion recently on the flow rates of the artificial bottle nipples, due to varying reports in some of the most recent articles published on flow rates. In fact, there is a newly released article from the United Kingdom. (Abstract link: https://doi.org/10.1080/2050571X.2019.1646463)
There has been much discussion recently on the flow rates of the artificial bottle nipples, due to varying reports in some of the most recent articles published on flow rates. In fact, there is a newly released article from the United Kingdom. (Abstract link: https://doi.org/10.1080/2050571X.2019.1646463)